Thyroid goiter, characterized by an enlarged thyroid gland, is a prevalent thyroid disorder with potential long-term consequences if left untreated. Timely diagnosis and appropriate treatment of thyroid goiters are crucial to prevent long-term complications and ensure optimal health outcomes. From thyroid function tests for accurate diagnosis to a range of available treatments, individuals with thyroid goiters have options for managing their condition.
Diagnosis of a Thyroid Goiter
Physical Examination:
Diagnosing a thyroid goiter often begins with a physical examination. Thyroid doctors palpate the neck to identify swelling or nodules in the thyroid gland. The size, consistency, and mobility of the thyroid are crucial indicators during this examination.1
Imaging Studies:
Ultrasound imaging is a common and first diagnostic tool to visualize the thyroid gland’s size, shape, and the presence of nodules. Other imaging modalities, such as CT scans or MRIs, may be employed to assess the extent of the enlargement and detect potential complications.2
Thyroid Function Tests:
Blood tests, including thyroid function tests measuring T3, T4, and TSH levels, help assess the thyroid’s hormonal activity. An imbalance in these hormones may indicate underlying thyroid dysfunction, aiding in the diagnostic process.3
Symptoms of a Thyroid Goiter:
Visible Swelling in the Neck:
One of the most noticeable symptoms of a thyroid goiter is the visible swelling in the neck. This can be seen as a lump or enlargement below the Adam’s apple and may be more apparent when swallowing.4
Difficulty Swallowing (Dysphagia) and Breathing (Dyspnea):
As a thyroid goiter enlarges, it can exert pressure on the esophagus and trachea, leading to difficulty swallowing and breathing. This may manifest as a feeling of constriction in the throat or shortness of breath.5
Voice Changes:
Pressure from an enlarged thyroid can affect the vocal cords, resulting in changes to the voice. Individuals may experience hoarseness or a raspy voice due to compression of the laryngeal nerves.6
Request an Appointment
Please note that although we strive to protect and secure our online communications, and use the security measures detailed in our Privacy Policy to protect your information, no data transmitted over the Internet can be guaranteed to be completely secure and no security measures are perfect or impenetrable. If you would like to transmit sensitive information to us, please contact us, without including the sensitive information, to arrange a more secure means of communication. By submitting this form you consent to receive text messages from CVI at the number provided. Msg & data rates may apply. Msg frequency varies. Unsubscribe at any time by replying STOP.
Treatments for a Thyroid Goiter:
Thyroid Hormone Replacement Therapy:
For cases where the thyroid goiter is associated with hypothyroidism, thyroid hormone replacement therapy may be prescribed. This treatment aims to normalize thyroid hormone levels and potentially reduce the size of the goiter.7
Radioactive Iodine Therapy:
Radioactive iodine therapy involves the administration of radioactive iodine, which is absorbed by the thyroid gland. This may resulting in long term hypothyroidism requiring long term hormone replacement. This targeted radiation can shrink the goiter, particularly if it is caused by overactivity in the thyroid.8
Surgery - Thyroidectomy:
Thyroidectomy, or surgical removal of part or all of the thyroid gland, may be recommended for large or obstructive goiters, or in cases where cancer is suspected. This may not be ideal in patients who are older or those that have extension of the tissue into the chest, which will require breaking of the chest bones during the operation. Total thyroidectomy may be necessary for some conditions, while partial removal is an option in others.9 Total thyroidectomy would require lifelong hormone replacement and has a longer recovery compared to other options.
Non-Surgical Radiofrequency Ablation (RFA):
This non-surgical treatment uses a special probe that is inserted into the goiter tissue. The probe then heats up the tissue rendering it inactive, over time this tissue is reabsorbed by the body resulting in volume shrinkage. Depending on the size, this may require several treatments. Read more here about the RFA procedure.


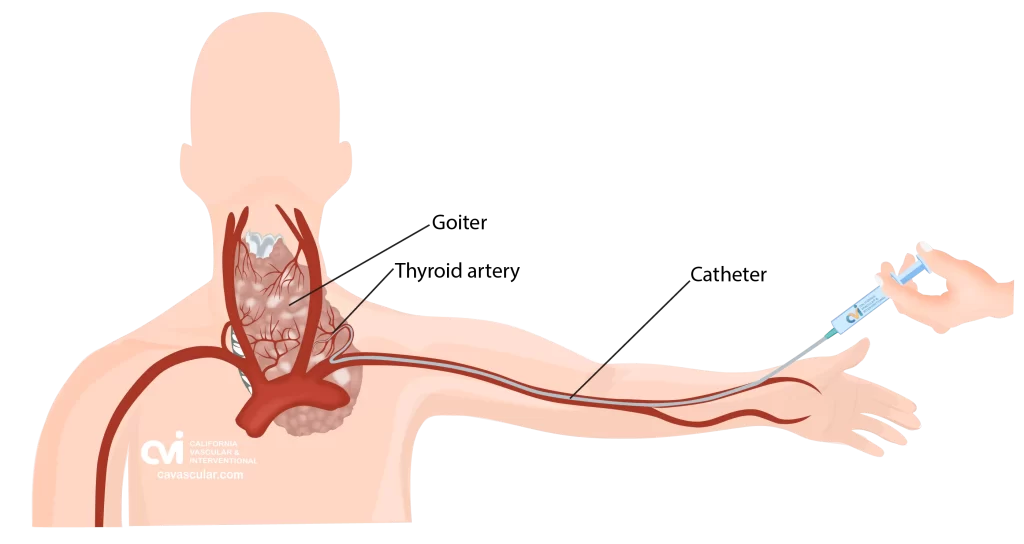
Non-Surgical Thyroid Artery Embolization (TAE):
Embolization has been around for many decades as a treatment modality for cancer, tumors, bleeding, pain etc. This method involves injecting tiny beads into the goiter tissue. Over time, the body resorbs the tissue that has lost its blood supply resulting in volume shrinkage. Read more here about the TAE procedure.
Long-Term Risks of Not Treating a Thyroid Goiter:
Without intervention, thyroid goiters can progress in size, leading to significant cosmetic concerns and compression of adjacent structures. Large goiters may cause difficulty swallowing (dysphagia), breathing problems, and a visible swelling in the neck. The longer the goiter remains untreated, the higher the risk of these complications.10
Progression of the Goiter:
One of the primary long-term risks of not treating a thyroid goiter is the progression of its size. Untreated goiters can continue to enlarge, leading to increased compression of nearby structures and potentially exacerbating symptoms.10
Effect on Thyroid Hormone Production:
Thyroid goiters can interfere with the normal production and regulation of thyroid hormones. As the gland enlarges, it may disrupt the synthesis and release of hormones, leading to an imbalance. This can result in hypothyroidism, characterized by symptoms such as fatigue, weight gain, and cold intolerance.11
Impact on Metabolic Health:
Persistent hypothyroidism due to an untreated goiter can have long-term consequences on metabolic health. It may contribute to dyslipidemia, insulin resistance, and an increased risk of cardiovascular diseases. Monitoring and managing thyroid function are crucial for preventing these metabolic complications.12
Compression Complications:
As a goiter enlarges, it can compress the trachea, leading to respiratory difficulties. Persistent compression of the esophagus may result in ongoing difficulty swallowing. These complications can significantly impact the quality of life.13
Thyroid Nodule Development:
Thyroid goiters left untreated may undergo nodular transformation, leading to the development of thyroid nodules. These nodules carry an increased risk of malignancy, and the longer the goiter remains untreated, the higher the likelihood of nodular formation.14
Impact on Quality of Life:
Untreated goiters that lead to persistent respiratory and swallowing complications can significantly impact a person’s quality of life. Difficulty breathing and swallowing can interfere with daily activities, sleep, and overall well-being. Addressing these issues early on is crucial for improving the long-term quality of life for individuals with thyroid goiters.15
Visible Disfigurement and Self-esteem:
A visibly enlarged thyroid goiter can lead to disfigurement, affecting an individual’s self-esteem and body image. Untreated goiters may cause psychological distress, anxiety, and depression, especially if the cosmetic concerns become more prominent over time.
Social Implications:
The psychological impact of an untreated thyroid goiter extends to social interactions and daily life. Individuals may experience social stigma or discomfort due to the visible swelling in the neck. Timely treatment can address these concerns and improve the mental well-being of affected individuals.16
Ignoring the potential long-term risks of untreated thyroid goiters can lead to progressive enlargement, compression complications, and an increased risk of thyroid nodules. Therefore, proactive medical intervention is essential for maintaining a healthy thyroid and overall well-being.
Thyroid Goiter: Surgery, Embolization or RFA
Surgery is a mainline treatment offered by an ENT surgeon for very large thyroid goiters or when cancer is suspected, but it requires general anesthesia, long recovery, possible surgical drains/tubes and leaves a scar.
For patients who want to avoid surgery, two minimally invasive options—thyroid artery embolization and radiofrequency ablation (RFA)—may be available. Each have a different approach, recovery and result. Embolization works by reducing blood flow to a larger thyroid area to shrink the gland, while RFA uses heat to shrink nodules or region of thyroid tissue reducing the size. Neither approach has major scars or incisions.
Studies have shown that RFA can reduce goiter volume by 50–90% over time with excellent safety and cosmetic results but requires multiple sessions. Thyroid artery embolization has also shown significant success, with studies reporting gland size reduction of up to 60%, improvement in thyroid labs, and symptoms like difficulty swallowing or pressure in the neck (Baek et al., 2021; Zang et al., 2020). Our doctor can help determine the best option based on your thyroid’s size, function, and symptoms.
Why California Thyroid Center?
Our physician is one of only a few specialists with a background in both thyroid RFA ablation and the embolization technique. He will evaluate you and decide which treatment option will suit you best. Sometimes a combination approach is necessary to save the thyroid gland.
Our center specializes in embolizations, and our staff is uniquely trained to care for these types of procedures, from the pre-op to the post-op period. Our specialist performs embolization for not only the thyroid but also in other higher risk and complex organs, such as the uterus, kidney, liver, prostate, lung and others. Patients are often surprised how quick and simple the TAE procedure was for them, but this comes at the experience of our specialist who performs a variety of complex embolizations safely. This diversity of experience has resulted in our specialist to treat complex cases safely and effectively.
Our specialist continually keeps up with the research to make sure that he brings the best and newest technology to our center. We are also always collecting feedback from patients and modifying how we provide care so that patients have the best level of experience.
Contact Us Today
Request an appointment to meet with our RFA specialist who will review your imaging, labs and history to determine if you are a good candidate for the procedure, and the outcomes you can expect. Each person is an individual and should discuss the potential risks and benefits of thyroid RFA with our doctor to decide if this is the best option.
Appointments are available via an online video telehealth platform or in person in Los Angeles, California. Why should you choose us? Read here.

1.) Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39-51.
2.) Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237(3):794-800.
3.) Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. JAMA. 2004;291(2):228-238.
4.) Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39-51.
5.) Brunn J, Block U, Ruf G, et al. Volumetric analysis of thyroid lobes by real-time ultrasound (author’s transl). Dtsch Med Wochenschr. 1981;106(41):1338-1340.
6.) Sturniolo G, Vermiglio F, Moleti M, et al. Voice changes during and after pregnancy. J Endocrinol Invest. 2012;35(4):383-387.
7.) Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association task force on thyroid hormone replacement. Thyroid. 2014;24(12):1670-1751.
8.) Brito JP, Gionfriddo MR, Al Nofal A, et al. The accuracy of thyroid nodule ultrasound to predict thyroid cancer: systematic review and meta-analysis. J Clin Endocrinol Metab. 2014;99(4):1253-1263.
9.) Hay ID, Johnson TR, Kaggal S, et al. Papillary thyroid carcinoma managed at the Mayo Clinic during six decades (1940-1999): temporal trends in initial therapy and long-term outcome in 2444 consecutively treated patients. World J Surg. 2002;26(8):879-885.
10.) Vanderpump MP. The epidemiology of thyroid disease. Br Med Bull. 2011;99:39-51.
11.) Brent GA. Mechanisms of thyroid hormone action. J Clin Invest. 2012;122(9):3035-3043.
12.) Pearce EN. Thyroid hormone and obesity. Curr Opin Endocrinol Diabetes Obes. 2012;19(5):408-413.
13.) Hegedüs L. The thyroid nodule. N Engl J Med. 2004;351(17):1764-1771.
14.) Fiore E, Vitti P. Serum TSH and risk of papillary thyroid cancer in nodular thyroid disease. J Clin Endocrinol Metab. 2012;97(4):1134-1145.
15.) Tan GH, Gharib H. Thyroid incidentalomas: management approaches to nonpalpable nodules discovered incidentally on thyroid imaging. Ann Intern Med. 1997;126(3):226-231.
16.) Sarlis NJ. Expression of the emotional distress and body image changes due to the presence of an untreated thyroid mass. Thyroid. 2004;14(12):1045-1047.
The above information explains what is involved and the possible risks. It is not meant to be a substitute for informed discussion between you and your doctor but can act as a starting point for such a discussion.